
You’ve got questions.
Maybe you’ve never been to therapy before. Maybe you’re wondering what emotionally-focused therapy is (or what the heck emotions are). Or what’s the difference between therapy and counseling, anyway?
Gotcha covered.
How much does therapy cost?
My standard fee is $150 for a 50-55 minute individual session. For couple/pair and family counseling, we will meet for 70-75 minutes at a fee of $185. You are responsible for paying at time of service unless we have made prior arrangements, such as check, cash, or electronic payment. I also am in-network with Premera, Lifewise, and Anthem insurance plans.
What about sliding scale therapy?
I accept a limited number of clients on a sliding scale basis for people experiencing economic hardship via Open Path Collective. Open Path charges a one-time fee of $65 that grants lifetime access to their network of sliding-scale providers; please see their website for more information on the fee.
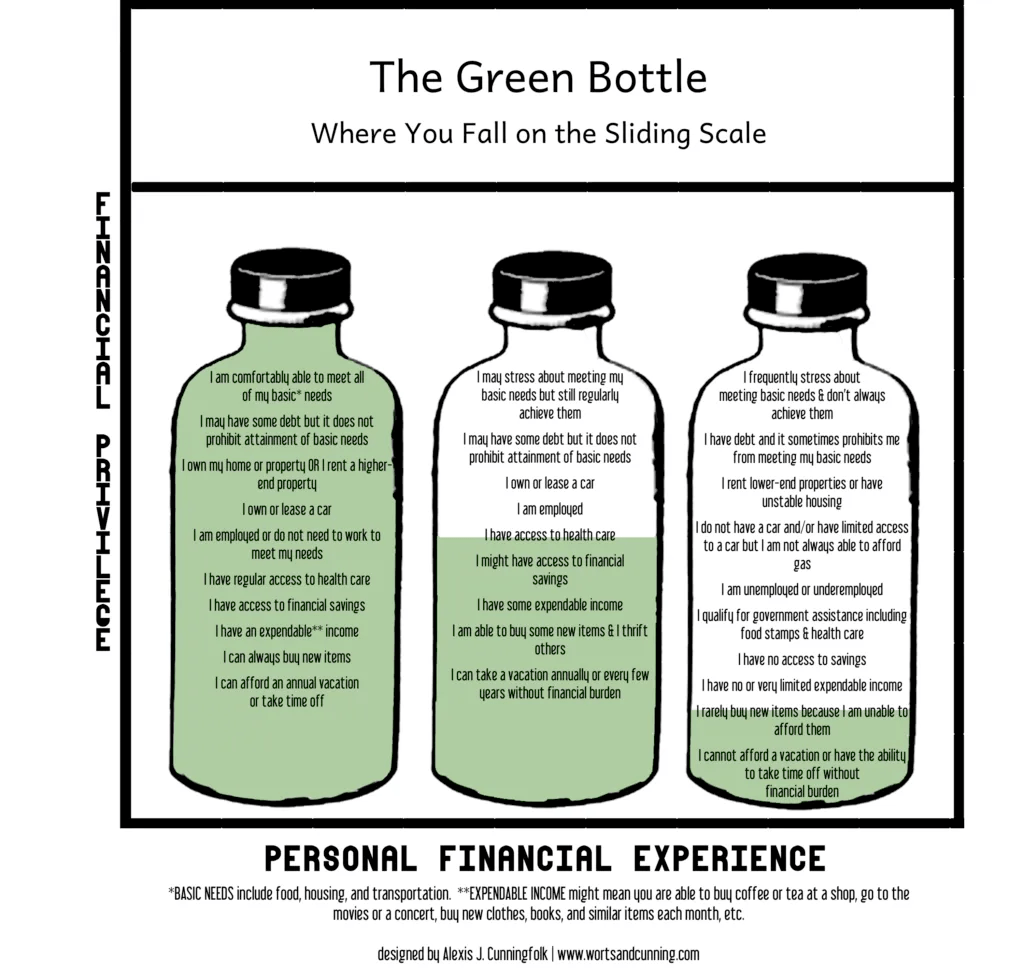
For clients with an Open Path member ID, I provide individual, couple/pair, and family counseling for a reduced fee. I reference the Green Bottle method from Embracing Equity and Alexis Cunningfolk for setting the scale. You choose the fee you pay, based on where you fall on the scale.
- Top of the scale/full bottle: $70 per 50-55min individual session; $80 per 70-75min relationship/family session
- Middle of the scale/half bottle: $55 per 50-55min individual session; $60 per 70-75min relationship/family session
- Bottom of the scale/low bottle: $40 per 50-55min individual session; $40 per 70-75min relationship/family session
When my OpenPath sliding scale spots are full, I offer sliding scale appointments at $80/individual session, $85/relationship/family session.
Can you provide fee transparency?
Sure! I charge market rate for my level of license and experience. This fee also allows me to offer 3-5 sliding scale spots for experiencing financial hardship. The session fee you pay goes to:
- paying for my time and expertise (I did go to grad school for this!) in the session with you
- completing notes and documentation after your session
- treatment planning before/after your session,
- performing research before/after your session
- my ongoing training and development via trainings, books, consultations, etc.
- supervision as required by the state
- rent
- insurance
- internet
- electronic health record platform
- website fees, and other monthly overhead expenses
- tissues.
What kind of therapist are you?
I am an integrative Relational-Cultural (RCT) therapist, which is the fancy way of saying that I believe that human beings grow through relationships with others, and that I draw from other therapy modalities based on your needs and goals.
I’m a therapist who will:
- Be curious about, and try to deeply understand, your lived experience and what makes you, you.
- See you as the expert on yourself.
- Collaborate with you on insights, tools, and new ways of being. I see therapy as something we do together.
- Challenge you and hold you accountable.
- Own when I make mistakes, and do my best to repair rupture with you.
- Continuously educate myself, not just on emerging theories and techniques, but also on the application of social justice, decolonization, and anti-oppressive practices within therapy and mental health counseling.
In my practice, I draw from:
- Emotionally Focused Individual (EFIT), Couple (EFCT), or Family (EFFT) Therapy (I am trained and recognized by ICEEFT as an EFIT and EFCT Therapist)
- Dialectical Behavior Therapy (DBT) or Radically-Open Dialectical Behavior Therapy (RO-DBT)
- Acceptance and Commitment Therapy (ACT)
- Parts work (similar to internal family systems, or IFS)
- Somatic-based practices
- Existential Therapy
- Strengths-Based Therapy
- Motivational Interviewing
I also practice embodied movement and meditation, use tarot cards for growth and development, and follow lunar and seasonal cycles to guide and connect to something larger than the self. If you are interested, I would be more than happy to discuss bodywork and spirituality in addition to “typical” counseling styles.
As your therapist, I see myself as your hermit guide: in the archetype, the hermit holds a lantern and stands alone on top of a mountain. The hermit represents deep, solitary introspection and emotional and spiritual growth. As your hermit guide, I will walk the path of life alongside you, holding the lantern: this will make it easier to see the path in front of us, and it is also my job to shine the lantern in areas of darkness you may be avoiding to help you move forward with less fear and more clarity. However, we walk the path together, so you will not be alone on this journey. You’ll see lanterns all over my practice.

What can I expect in therapy?
The first two or three sessions will feel a bit like an interview. This process is called intake. During intake, I’m gathering information, understanding how you think and see the world, and feeling what it’s like to really be you. I’m also assessing, especially if a diagnosis is required. I’m getting a sense of what goals we might take, and what we might do together to help you get to where you want to be.
Next, we might treatment plan, depending on your goals and needs. This might be formal (written down, tracked, measured), or informal (named between the two of us, noted and checked in on casually), or somewhere in between. Intake and treatment planning might take 3-5 sessions, depending on your needs and goals.
Then comes the work (although we’ve been doing a bit of this the whole time). This is where we’ll spend most of our time in therapy together. This looks like trying new things, excavating layers of stories and coping/ defense mechanisms, and seeing what change and possibility exists in the newly-found space, giving and receiving feedback, going back to the drawing board, and being curious about yourself and your experience. Over and over (and over) again. Throughout, we’ll together be assessing and tracking progress toward goals, either formally or informally. The work might take 10 to 20 sessions, or it might take upwards of a few years, depending on your needs and goals.
Finally comes termination, in which we’ll bring our work together to a close. This can take 1 to 3 sessions. We’ll summarize our work together, highlight your progress, and share thoughts on where next areas of work might lay. We will also process and reflect on our time together and the therapeutic relationship we built.
I am a relational- and systems-oriented therapist. We might discuss the ways the two of us work together in our therapeutic relationship and how this might apply to other relationships in your life; where you might be facing challenges in personal or professional relationships; and how you relate to the broader systems of society (e.g. patriarchy and white supremacy, capitalism, individualism and community), and how all of these relationships and systems impact your well-being and goals.
You don’t look like me. How will you understand me?
I’m yet another cisgender, femme, straight-size, het-presenting white woman therapist. I don’t blame you if you have your doubts about me. And you’re right — I haven’t lived in your skin. I don’t know what it’s like to be you. But it is my job (and my passion) to listen, and strive to understand.
In order to do this well, that means I have to do (and do) my homework, and my own personal racial reckoning work. This is an ongoing and lifelong process, and I value this work greatly. I am always open to feedback about my own blind spots, and where there is more work I need to do. Please point such blind spots out if you encounter them, but the work to educate me is not yours. I own that.
And. No matter how much I know about your identities or culture broadly, and while it will give me context, it doesn’t tell me your experience. What it’s like to be uniquely, exquisitely, you, in your world. You are the expert on you, and I will need your help to understand what that feels like.
What if I leave session angry, uncomfortable, upset, or mad at you?
Well, that’s to be expected sometimes, I’m afraid. The goal of mental health counseling is to improve your well-being over time, not necessarily to leave every session “feeling better.” And, I ascribe to the belief that the point of life is not to avoid all pain; it’s to experience life and live despite the pain.
To live is to suffer; to survive is to find some meaning in the suffering.
Gordon Allport, in the 1962 introduction to Viktor Frankl’s Man’s Search for Meaning
So therefore, avoiding anger and discomfort isn’t the point — it’s getting comfortable with experiencing those feelings and living a life aligned with your values, despite your discomfort or anger.
And, our emotions tell us something. If you’re angry, uncomfortable, upset, or mad at me, we might be touching on some very important topics for us to cover. That doesn’t mean we should rush into them; the emotions are just useful data that we can notice. I also might be inviting you to sit in uncomfortable feelings or memories, which, in turn, might cue your body to send you messages or feelings of discomfort or danger. That doesn’t mean those feelings are wrong. They could be a sign for us to slow down. Letting me know about those feelings can help me pace our work better.
Finally — I’m a human being. Chances are good that, over our time together, I will wish I would have done something differently: something landed poorly, I put my foot in my mouth, I forgot your partner’s/parent’s/pet’s name…and you would be well within your rights to be angry, uncomfortable, upset, or mad at me! Rupture and repair are an invaluable component of the therapeutic relationship; research shows our relationship will become stronger and our work will become more effective if we can find a way to move through difficult moments together. I invite and encourage you to share those feelings with me.
Will you diagnose me?
If you are using your insurance or providing a superbill to your insurance provider to obtain reimbursement for therapy, I am required to provide a diagnosis on the claim/superbill, and thus am required to diagnose you. If I am required to diagnose you, I will educate you on your diagnosis.
I otherwise am neutral on diagnosing. For some clients, having a diagnosis can provide answers, open the doors to resources or remove barriers to access, or build bridges to community. For others, a diagnosis can be a label that can come with stigma (internal or external), and/or real-world implications.
I take diagnosing seriously. If you think you should be diagnosed with something, let’s talk about it. If you’re curious what I would diagnose you with, let’s talk about it. If you very much don’t want to be diagnosed, let’s talk about it.
The therapy modalities I practice are trans-diagnostic; that means we look at what you’re experiencing, what’s working, and what’s not. We’ll maybe build skills, or maybe build an entirely new way of thinking. So does it matter if you’re diagnosed with Generalized Anxiety Disorder if what we’re doing is reducing what you’re actually experiencing? For some, the answer is yes; for others, no. So, let’s talk about it.
Can you diagnose me with ADHD or autism?
Washington is not a state that limits the diagnostic capabilities of licensed mental health counselors, so I am able to diagnose attention deficit/hyperactive disorder or autism spectrum disorder. It does not mean the diagnosis will be accepted by an employer, the government when seeking accommodations, or a medical provider, especially when seeking medication. These entities may require a diagnosis to be made by a medical doctor, a psychiatrist, or a psychiatric nurse practitioner to be considered “valid.”
Further, I am not a trained assessment provider for ADHD or autism spectrum disorder. We can certainly discuss these (or any) diagnoses, do some preliminary assessments, and figure out, based on your goals and needs, where to go from there.
Can you prescribe medication?
Licensed mental health counselors/associates cannot prescribe medication. If you, or we, think medication should be considered, we will need to work with, or find you, a primary care provider, a psychiatrist, psychiatric nurse practitioner, etc. See Washington state’s list of providers who can prescribe for more information.
Are you trauma-informed?
Yes. Relational-Cultural Therapy (RCT) and Emotionally-Focused Therapy (EFT) are, by nature, trauma-informed. I practice trauma-informed versions of ACT and DBT, including RO-DBT. Depending on your goals and needs, we may discuss things that happened to you, how their echoes have reverberated through your life, and methods by which you can carry your burdens a little more easily. However, you are in charge of how quickly, or if, we even look at those things. It is deeply important to me that you feel safe in our therapeutic relationship so we don’t excavate too much, too soon.
That doesn’t mean that you won’t sometimes feel uncomfortable in session. In our work together, we may talk about things that are challenging, emotional, and sometimes require a great deal of vulnerability. I might be inviting you to sit with feelings, memories, or thoughts that you have repressed, forgotten about, or intentionally buried.
You might leave a therapy session feeling depressed, anxious, drained, emotional, or angry. As your therapist, it is my job to help you sit with and process those feelings, such that you can better hold the entire emotional experience of the human existence. The goal of mental health counseling is to improve your well-being over time, not necessarily to leave every session “feeling better.”
You might even subconsciously feel I’m a threat to your (emotional) safety, because we’re touching on difficult topics and coming up against coping and defense mechanisms that you’ve built for a good reason, even if they’re not serving you now. I hope that, by naming it in advance, you feel comfortable bringing the topic up so that we can work through it together.
What is trauma?
A “traumatic event” is one that involves a significant degree of actual or threatened physical or psychological harm, to oneself or others. This can include everything from genocide, miscarriage, or bullying, to murder, abuse, and mass shootings; from divorce, death, or disaster, to violence, rape, and torture; from car accidents, injuries, and illnesses to the medical or surgical treatments for those things. It may also include incidents where people instigate, perpetrate, fail to prevent, or witness actions that violate or contradict their own moral code.
A “trauma-related disorder” involves: 1) direct or indirect experience of traumatic events; 2) distressing emotional, cognitive, and physiological reactions to that experience; and 3) the inability to cope effectively with one’s own distressing reactions.
Is there risk in using my insurance?
Accepting insurance makes mental health counseling more accessible, which is critical to both individuals and our communities. However, using insurance for mental health services comes with risk: using insurance requires a diagnosis, and potentially for me to disclose information about you. If I am required to diagnose you, I will educate you on your diagnosis.
Some diagnoses (like Borderline Personality Disorder) can carry an unfair societal stigma, and may impact other medical services you receive, or how other providers perceive you. Clients should be aware that the current political administration is changing mental health laws day-to-day, and carrying a diagnosis may come with risk(s) yet unknown.
I can provide you with a superbill, which you can then provide to your insurance provider for reimbursement. Superbills must be agreed to in advance. Check with your insurance provider if they will accept a superbill from an out-of-network clinical mental health counselor.
What is a superbill?
A superbill is a receipt from your therapist provided to you after a session has occurred. You pay the session fee to your therapist; you can then submit your superbill to your insurance carrier for potential out-of-network reimbursement directly.
For successful claims processing with your insurance, the superbill must contain at least:
- your name, date of birth, and insurance ID number
- the date of service for the session
- the CPT code for the session (for most therapy sessions this is 90791, 90837, or 90834), including any modifiers for the session if it was a telehealth session
- your diagnosis (yes, even with out-of-network billing, you must have a diagnosis on the superbill for insurance reimbursement)
- my name, license number, NPI number, and tax ID number
- the fee for the session, and how much you paid
Some insurers may require more information on a superbill, but this is typically what is required.
What’s the difference between psychotherapy, therapy, and counseling?
Not much. One way to think of it is: therapist (mental health) is a job title and what I do, counselor is a license (I am a licensed mental health counselor; I practice psychotherapy). Some people will say that counseling is focused on a specific issue, or is short-term in practice. Therapy is a broad field which can include things like physical therapy and massage therapy, as well as psychotherapy, or what people typically think of when they hear therapy of the mental health variety, so there’s a push within the counseling field to use more precise language (e.g. mental health counseling).
However, social workers, marriage and family therapists, and psychologists can also provide mental health counseling/psychotherapy, and don’t want to call themselves counselors because…they’re not counselors. So the language gets confusing, but you’ll generally hear mental health counseling, therapy, and psychotherapy used interchangeably.
Depending on your goals, we might do short-term, issue-focused counseling. Or, we might do deeper-level, psychotherapeutic work focusing on understanding who you are, how you came to be, and how to get to where you want to go in life.
Why is your practice called “Aspen Stand”?
An aspen stand may contain thousands of trees, but they’re actually one organism — they’re all connected underground. In much the same way, we’re all members of community and society, and, for some of us, our work is learning how to tap back into those roots.
I also grew up surrounded by aspen trees in rural Montana. They are a beautiful marker of the seasons: barren branches draped in icicles after an ice storm; the puffs of catkins then vibrant green leaves in the first hints of spring (when everyone wears shorts as soon as it’s above 40° in March!); the stark contrast between the black and white bark and silver-green leaves, combined with the rustling of the leaves, delights the senses in full summer. Then, finally, the breathtaking blaze of orange and yellow for the precious few weeks in the fall, before the leaves somehow overnight brown and deaden, falling to the ground. Just as it seems the light will never return, the cycle begins anew.
Aspen trees remind us that everything has its rhythms, and nature is inevitable. Life is fleeting and ephemeral; all we can do is live fully.
What trainings have you taken recently?
- Emotionally Focused Couples Therapy Externship (July 2025)
- Emotionally Focused Individual Therapy Essentials (Levels 1-2) (July 2025)
- Fundamentals of Emotionally Focused Counseling (May 2025)
- Tarot & Therapy: Intuition and Metaphor (June 2024)
- Gottman Level 1 Couples Counseling (May 2024)
What have you read lately?
- Fearing the Black Body: The Racial Origins of Fat Phobia: Sabrina Strings
- Trauma-Focused Acceptance and Commitment Therapy: Russ Harris
- The Body is Not an Apology: The Power of Radical Self Love: Sonya Renee Taylor
- Attachment Theory in Practice: Sue Johnson
- My Grandmother’s Hands: Racialized Trauma and the Pathway to Mending Our Hearts and Bodies: Resmaa Menakem
- A Primer for Emotionally-Focused Individual Therapy (EFIT): Sue Johnson & T. Leanne Campbell
- The Practice of Emotionally Focused Couple Therapy: Sue Johnson
- Maybe You Should Talk to Someone: Lori Gottlieb
What are emotions?
Emotions are something totally normal and natural to have; they’re not wrong or bad. Everyone has them (even you! You just might have learned really early on how to shut them down, to keep yourself safe). They’re nothing bad in and of themselves—they’re there for a reason!
Experts say there are core emotions; just how many varies (anywhere from 4-8). An easy way to remember a few are the (a)s: mad, sad, glad, and afraid.
Emotions exist to keep us safe (especially emotions like fear, anger, and shame). They motivate us to do something! In the case of fear, to run; anger, to attack; and shame, to hide. And contrary to popular belief, the idea is not to change emotions, or not feel them; the idea is to learn how to hold them and still live your life. They are a natural part of the human experience; shutting them down or denying them only makes things worse in the long run.
Check out the Feelings Wheel for a great visual.
